Question: I’m a provider and am aware that there have been new developments in cervical cancer screening technologies. How do the updated guidelines take these developments into account, and how do they affect my practice?
Dr. Michael Policar responds: Since the publication of the updated chapter on Screening for Cervical, Ovarian, and Breast Cancer in Contraceptive Technology (22nd edition),1 there have been four new developments in cervical cancer screening, moving us closer to personalized management: primary HPV screening for average risk patients, self-sampling for some people, dual staining of cytology samples, and extended HPV genotyping. Clinicians need to be aware of the updates in national guidelines, and in some cases, utilize these new technologies, depending on the logistics of cervical cancer screening in your practice.
- In December 2024, the US Preventive Services Task Force (USPSTF) published a draft of their Recommendation Statement on Cervical Cancer: Screening2. The statement has two important new components for screening persons 30 to 65 years of age:
- Primary HPV screening (with a high-risk HPV test-alone) every 5 years as the preferred screening strategy in this age group
- Obtaining a clinician- or a patient-collected high-risk human papillomavirus (HPV) sample.
- The ASCCP published three new guidelines in the Journal of Lower Genital Tract Disease based on recommendations written by the Enduring Consensus Cervical Cancer Screening and Management Guidelines Committee: (1) self-collected vaginal specimens for HPV testing3 (April, 2025) (2) recommendations for the use of p16/Ki67 Dual Stain4 (April, 2024), and (3) applying results of extended genotyping to management of positive cervicovaginal HPV test results5(April, 2025).
Primary HPV Screening
Earlier versions of the USPSTF guidelines (most recently in 2016), recommended 3 co-equal options in screening for cervical cancer in women 30-65 years of age: cytology every 3 years, co-testing (cytology and an HPV test ) every 5 years, and HPV-alone (primary screening) every 5 years. In the 2024 USPSTF draft, HPV-alone screening is given top billing, based upon comparison of the benefits (preventing cervical cancer cases and deaths) and the harms (false positives leading to unnecessary colposcopy and treatment) of each approach. Meta-analyses showed that while all three approaches led to similar profound reductions in cervical cancer cases and deaths, primary HPV screening resulted in fewer tests performed and fewer colposcopies, but slightly more cancers per 1,000 women over a lifetime when compared to co-testing. However, given similar benefits, the guideline stated that as an alternative to primary HPV screening, continued screening with cervical cytology alone every 3 years or screening with co-testing every 5 years is acceptable. Note that these guidelines apply only to average-risk patients, which is defined as not having a medical condition that causes immunocompromise, no history of in-utero DES exposure, and no history of CIN 2+ in the past 25 years.
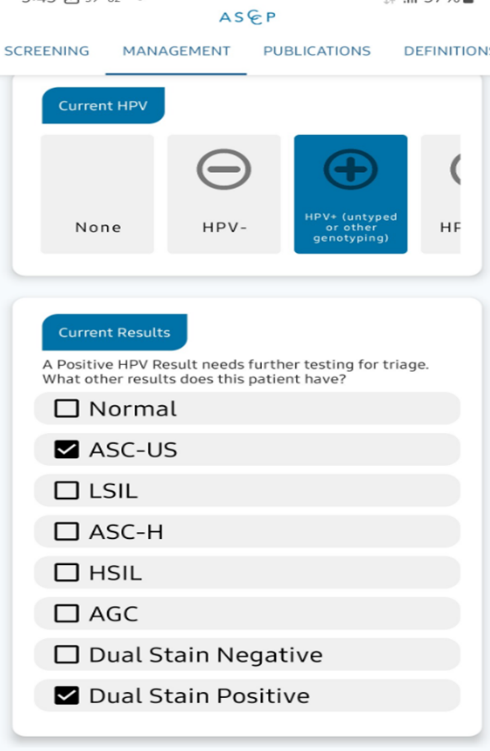
Every clinician who performs cervical cancer screening should be familiar with the ASCCP Management Guidelines app, which can be purchased for $14.99. The same information is available for free from the ASCCP website at https://www.asccp.org/mobile-app. The management guidelines contained in the app have been updated to provide advice to clinicians regarding the management of clients with a positive HPV test and the reflex cytology that is performed in the same lab
Self-sampling3
Self-sampling for HPV in order to screen for cervical cancer precursors has been a topic of interest for decades, as this approach is likely to improve screening rates in people who prefer to avoid a clinician-performed speculum exam and for those unable or unwilling to be evaluated in a clinical setting. Precedent exists for successful self-sampling for other lower genital tract pathogens (e.g., obtaining gonorrhea and chlamydia specimens for nucleic acid amplification tests).
Studies in Europe and the US have shown that self-collected HPV tests are slightly less sensitive than clinician-collected tests (relative sensitivity, 0.91-0.94). Consequently, the Enduring Consensus Guideline2 stated that while clinician-collected cervical specimens are preferred, self-collected vaginal specimens are acceptable for primary HPV screening of asymptomatic average-risk individuals as defined above. Given the drop-off in sensitivity, repeat testing in 3 years, rather than the usual 5 years, is recommended following HPV-negative screens using self-collected vaginal specimens. Minimal data regarding surveillance following abnormal screening test results, colposcopy, or treatment are available, and therefore, clinician-collected cervical specimens are preferred in these circumstances.
This recommendation applies only to tests with an FDA indication for primary HPV screening using self-collected vaginal specimens. These include the BD Onclarity HPV Assay with the Copan 522C.80 swab and the Roche cobas assay with Evalyn brush or Copan 522C.80 swab. If not supplied by the pathology lab that your practice uses, the Copan swabs can be purchased for about $1 each and the Evelyn swab costs about $6 each. Meta-analyses show a high level of acceptability and preference for self-collection over clinician sampling (ease and privacy)6 and increased screening rates compared with an invitation to clinic (12% absolute increase)7 ,
At this time, self-collection devices are FDA-approved only for use in medical settings, including clinics, offices, mobile vans, urgent care centers, etc., but not for home collection because there are not yet adequate studies to validate home collection. However, one study done in North Carolina using home self-collection shows that this approach is acceptable for clients and may make home sampling more cost-effective than clinic-based collection for detection of CIN2+8
Important caveats regarding HPV self-collection
- If you plan to start the self-collection option in your clinic or office, check to make sure that your path lab is using either the BD Onclarity or the cobas test and that the appropriate collection swabs are used.
- Self-collection applies only to the 30-65 age group, as persons 21-29 are still screened with cytology alone every 3 years.
- The published guidelines do not apply to self-sampling at home or non-clinical settings…yet. However, outside of the guidelines, a number of companies offer home HPV collection kits that can be purchased online, including the costs of transferring the sample to a lab, the performance of the HPV test, and providing the client with the test results. Most of these products require the client to pay out-of-pocket and they are not covered by Medicaid, state family planning programs, or commercial health insurance at this time.
Dual Staining4
In 2020, the US FDA approved the use of p16ink4a/Ki-67 dual stain (DS) for cytology samples to inform the management of those with a positive HPV test. These stains check for activity of p16, (a tumor suppressor protein which reflects HPV-related oncogene activity) and Ki-67 which is a marker of cell proliferation. Detection together in the same cell is strongly associated with precancerous cellular changes (CIN3+). Not all pathology laboratories perform this test…check to determine whether it is available to your clients in the lab that you use, whether the test is done at the discretion of the pathologist or if it has to be ordered separately, and whether it is a benefit of the client’s health plan or payer.
In general, HPV+/DS+ will prompt colposcopy; HPV+/DS- will prompt return in one year. Note that dual staining results are included in the ASCCP app so that you won’t have to look up management recommendations when this test has been performed in the lab
However, if you don’t have the app available or need more detailed management information, the table below is excerpted from the Enduring Guidelines5 article by Massad in the Journal of Lower Genital Tract Disease.
| Current HPV | Current DS result | Past history | Management | |
|---|---|---|---|---|
| HPV 16/18 | 16 and/or 18 | N/A1 | N/A | Colposcopy with collection of cytology if available |
| HPV 45, 33/58, 31, 52/35/39/68, 51
Untyped or “other” types when 16 or 18 are not present |
45, 33/58, 31, 52/35/39/68, 51 or untyped/other | DS Positive2 | N/A | Colposcopy |
| 45, 33/58, 31, 52/35/39/68, 51 or untyped/other | DS Negative3 | Normal4 or colposcopy <CIN25 within past 1 year | Repeat HPV test in 1 year | |
| 45, 33/58, 31, 52/35/39/68, 51 or untyped/other | N/A | HPV+ without colposcopy (i.e. current test is 2nd consecutive HPV+) | Colposcopy | |
| HPV 59/56/66 | 59/56/66 | N/A | Normal or colposcopy <CIN2 within past 1 year | Repeat HPV test in 1 year2 |
| 59/56/66 | N/A | HPV+ without colposcopy (i.e. current test is 2nd consecutive HPV+) | Colposcopy |
Extended genotyping5
Currently, six different high risk HPV screening tests are commercially available in the US: Hybrid Capture 2, Cervista, Aptima (E6/E7), cobas, BD Onclarity, and Alinity . Only cobas, BD Onclarity and Alinity are FDA cleared for primary screening, while the others are approved for co-testing and triage of ASC-US cytology results. Each one tests for 13 or 14 high-risk HPV types; some also test for specific high-risk types (16, 18, 18/45). Some laboratories have developed their own “in-house” (or “home-grown”) HPV genotyping tests that have not been reviewed by the FDA, making it difficult to comment on their accuracy.
We now know that the “12 other” high-risk HPV types, when present or absent, have the potential to further stratify patients into risk categories. Two FDA-cleared assays provide extended genotyping of specific HPV types: the Onclarity HPV Assay (approved April 2020) and the Alinity m High-Risk HPV Assay (approved November 2023). Extended HPV genotyping results are interpreted in the context of current and prior cytology and/or dual stain results. In general, extended HPV genotype test results indicating relatively higher risk HPV strains will lead to colposcopy in some persons with minimally abnormal cytology who would otherwise have had repeat testing in 1 year
Results of extended genotyping (beyond HPV 16, 18, and 45) are not included in the ASCCP app. Detailed management information, based on current HPV type (from extended HPV genotyping) and current and past cytology results, are included in the table below, which is excerpted from the Massad Enduring Guidelines5 article.
| Current HPV | Current cytology | Past results | Management | |
|---|---|---|---|---|
| HPV 16/18 | 16 | HSIL1 | N/A2 | Treatment preferred; colposcopy acceptable |
| 16 | ASC-H3 | N/A | Treatment or colposcopy | |
| 16 | NILM4, ASC-US5, LSIL6, AGC7, or no cytology | N/A | Colposcopy8 with collection of cytology if not already done | |
| 18 | HSIL | N/A | Treatment or colposcopy | |
| 18 | NILM, ASCUS, LSIL, ASC-H, AGC, or no cytology | N/A | Colposcopy8 with collection of cytology if not already done | |
| HPV 45, 33/58, 31, 52/35/39/68, 51
Untyped or “other” types when 16 or 18 are not present |
45, 33/58, 31, 52/35/39/68, 51 or untyped/other | HSIL, ASC-H, AGC | N/A | Colposcopy8,9 |
| 445, 33/58, 31, 52/35/39/68, 51 | ASC-US or LSIL | N/A | Colposcopy | |
| Untyped/other | ASC-US or LSIL | Documented HPV negative screen in past 5 years or colposcopy <CIN210 in past year | Repeat HPV test in 1 year | |
| Untyped/other | ASC-US or LSIL | Any history other than above | Colposcopy | |
| 45, 33/58, 31, 52/35/39/68, 51 or untyped/other | NILM | Normal11 or colposcopy | Repeat HPV test in 1 year | |
| 45, 33/58, 31, 52/35/39/68, 51 or untyped/other | N/A | HPV+ without colposcopy (i.e. current test is 2nd consecutive HPV+) | Colposcopy | |
| HPV 59/56/66 | 59/56/66 | ASC-H, AGC, or HSIL12 | N/A | Colposcopy8 |
| 59/56/66 | NILM, ASC-US, LSIL or no cytology12 | Normal or colposcopy | Repeat HPV test in 1 year | |
| 59/56/66 | N/A | HPV+ without colposcopy (i.e. current test is 2nd consecutive HPV+) | Colposcopy |
In summary, these advances move us even closer to “personalized management” based on abnormal cervical cancer screening results. However, it’s important to make sure that these interventions are implemented in collaboration between your practice and the pathology lab that your practice works with.
References
- Policar MS, Sawaya GF, Cason P. Screening for cervical, ovarian, and breast cancer. In: Cason P, Cwiak C, Edelman E, et al. (Eds) Contraceptive technology, 22nd edition. Burlington,MA: Jones-Barlett Learning, Inc., 2023.
- https://www.uspreventiveservicestaskforce.org/uspstf/draft-recommendation/cervical-cancer-screening-adults-adolescents
- Wentzensen N, Massed LS, Clarke MA, et al. Self-Collected Vaginal Specimens for HPV Testing: Recommendations from the Enduring Cervical Cancer Screening and Management Guidelines Committee. J Low Genit Tract Disease April 2025; 29(2):144-151
- Clarke MA, Wentzensen N, Perkins R, et.al. et al. Recommendations for the Use of p16/Ki67 Dual Stain for Management of Individuals Testing Positive for HPV. J Low Genit Tract Disease April 2024; 28 (2):124-130
- Massad LS, Clarke MA, Perkins R, et.al. Applying Results of Extended Genotyping to Management of Positive Cervicovaginal HPV Test Results: Enduring Guidelines. J Low Genit Tract Disease April 2025; 29(2):134-143
- Nelson EJ, Maynard BR, Loux T, et.al. The acceptability of self-sampled screening for HPV DNA: a systematic review and meta-analysis. Sex Transm Infect 2017 93(1):56-61;
- Verdoodt F, Jentschke M, Hillemanns P, et.al. Reaching women who do not participate in the regular cervical cancer screening programme by offering self-sampling kits: a systematic review and meta-analysis of randomised trials. Eur J Cancer . 2015 Nov;51(16):2375-85. doi: 10.1016/j.ejca.2015.07.006. Epub 2015 Aug 18.
- Pretsch PK, Spees LP, Brewer NT. Effect of HPV self-collection kits on cervical cancer screening uptake among under-screened women from low-income US backgrounds (MBMT-3): a phase 3, open-label, randomised controlled trial. Lancet Public Health. 2023 Jun;8(6):e411-e421. doi: 10.1016/S2468-2667(23)00076-2. Epub 2023 May 11.
Other Latebreakers
Mar. 05, 2026
Abortion considerations when no yolk sac is detected
Other Latebreakers
Jan. 08, 2026
There’s no possible way I could be pregnant!
Other Latebreakers
Nov. 01, 2025
Answering your questions about wellness exams for adults assigned female at birth – often called the “well woman exam”
Other Latebreakers
Sep. 05, 2025
Acute Heavy Menstrual Bleeding!
Other Latebreakers
Aug. 01, 2025